Understanding Extreme Intestinal Expansion
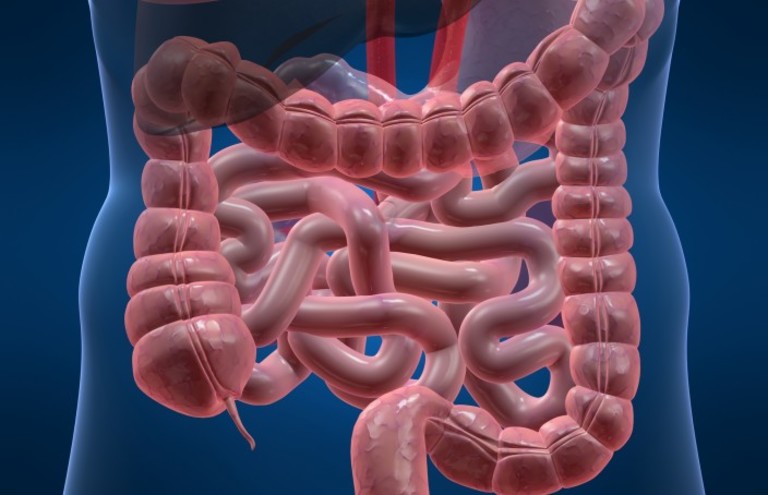
The human digestive tract is an incredibly adaptive and resilient system. However, when regular elimination patterns are disrupted for prolonged periods, the large bowel can undergo severe anatomical transformations. The medical imaging provided highlights an extreme instance of colonic expansion, historically referred to in clinical literature as a megacolon or severe fecal impaction.
When a person experiences severe abdominal retention that lasts for weeks, months, or even years, the structural integrity of the bowel wall changes. Understanding why this happens, how the body reaches this state, and what medical interventions are required is essential for identifying early warning signs before the condition becomes a medical emergency.
What Happens Inside the Body During Chronic Impaction?

To understand how the large bowel reaches the massive proportions seen in the imaging, it helps to examine the mechanics of digestion. Under normal conditions, the large bowel absorbs water from digested food material and uses coordinated, rhythmic muscular contractions called peristalsis to move waste toward elimination.
When peristalsis fails or when waste material is consistently held back, the body continues to extract moisture from the retained material. This leads to a cycle of structural changes:
-
Dehydration of Waste: As waste remains stagnant, the lining absorbs excessive water, turning the material dense, hard, and deeply compacted.
-
Loss of Muscular Tone: The smooth muscles surrounding the large bowel stretch to accommodate the buildup. Over time, like an overinflated balloon, the muscle fibers lose their elasticity and their ability to contract.
-
Nerve Desensitization: Chronic stretching desensitizes the local nerve networks (the enteric nervous system). The brain stops receiving the clear signals required to trigger a natural bowel movement, leading to a complete reliance on external interventions.
Common Root Causes Behind Severe Colonic Expansion
An extreme presentation of abdominal distension and retention rarely happens overnight. It is typically the culmination of long-standing structural, neurological, or functional issues. Medical professionals categorize these causes into a few primary areas.
1. Congenital Conditions (Adult-Onset Hirschsprung’s Disease)
While typically diagnosed in infancy, mild forms of Hirschsprung’s disease can occasionally go undetected until late adolescence or early adulthood. This condition occurs when a person is born lacking necessary nerve cells (ganglion cells) in the distal segment of the large bowel. Without these nerves, that specific segment remains permanently narrow and tightly contracted, creating a functional wall that blocks anything from passing through. Material backs up behind this narrow segment, causing massive dilation over time.
2. Idiopathic Megacolon
When a thorough medical evaluation rules out any missing nerve cells, mechanical blockages, metabolic issues, or systemic diseases, the condition is classified as idiopathic. This means the underlying cause of the severe slow-transit retention remains unknown. It is often linked to a baseline, systemic dysfunction in how the smooth muscles or the local nervous system coordinates movement.
3. Neurological and Systemic Disorders
The digestive tract relies heavily on communication with the central nervous system. Conditions that disrupt nerve pathways can severely impact motility. These include:
4. Medication-Induced Motility Slowdown
Certain pharmacological agents heavily suppress the natural movement of the digestive tract. When taken chronically without proper medical management, they can contribute to severe impaction. Common culprits include heavy pain management therapies, certain psychiatric medications, and old-generation antihistamines.
Key Differences Between Functional Retention and Structural Megacolon

It is vital to differentiate between standard, uncomfortable functional retention and a true structural megacolon.
| Feature |
Standard Functional Retention |
Structural Megacolon / Severe Impaction |
| Duration |
Transient (a few days to a week) |
Chronic, progressive over months or years |
| Anatomical Diameter |
Normal to slightly distended |
Drastically widened (often exceeding 6 to 12 centimeters) |
| Response to Treatment |
Resolves with dietary changes or standard over-the-counter options |
Refractory to standard options; requires prescription or surgical care |
| Associated Symptoms |
Mild bloating, temporary straining |
Severe distension, inability to pass gas, nausea, paradoxical liquid leakage |
The Warning Signs That Demand Immediate Medical Evaluation
Many individuals quietly live with digestive discomfort, relying on self-treatment for long periods. However, ignoring progressive symptoms can lead to life-threatening complications. A medical evaluation is strictly necessary if regular symptoms are accompanied by any of the following warning signs:
-
Visible Abdominal Distension: The abdomen becomes noticeably firm, distended, and protruding, resembling a late-stage pregnancy or a severe ballooning effect.
-
Inability to Pass Gas (Flatus): A complete lack of gas movement indicates a total structural or functional blockage in the system.
-
Paradoxical Diarrhea: This occurs when liquid waste bypasses a massive, solid, impacted mass further up in the tract, giving a false impression of loose stools while the core blockage remains.
-
Persistent Nausea and Vomiting: When the lower digestive tract is completely blocked, waste and pressure back up into the upper GI tract, inducing systemic distress.
-
Systemic Signs of Distress: Fever, rapid heart rate, or sudden, sharp, localized abdominal pain can indicate that the bowel wall is losing its blood supply or is at risk of structural failure.
How Medical Professionals Diagnose and Assess the Condition
To determine the exact scale of colonic expansion and identify the underlying cause, medical teams utilize a precise diagnostic pathway.
Plain Abdominal Radiography (X-ray)
As demonstrated in the provided imaging, a simple, non-invasive abdominal X-ray serves as an initial diagnostic tool. It easily reveals the presence of massive loops of gas and dense waste material filling the abdominal cavity, outlining the exact paths of the dilated bowel segments.
Computed Tomography (CT) Scan
A CT scan provides cross-sectional, high-resolution views of the abdomen. This imaging modality allows specialists to view the thickness of the bowel wall, check for signs of hidden perforation or compromised blood flow, and pinpoint the exact location of the transitional zone between healthy and dilated tissue.
Anorectal Manometry
This specialized functional test measures the pressure and contractility of the rectal muscles and anal sphincters. It is highly useful for checking whether the normal relaxation reflex occurs when pressure is applied. A lack of this reflex heavily points toward a neurological or congenital issue like Hirschsprung’s disease.
Tissue Biopsy
The definitive method to rule out congenital conditions in adults is a full-thickness or suction rectal biopsy. Pathologists examine the tissue under a microscope to confirm the presence or complete absence of vital ganglion cells within the nerve plexuses of the bowel wall.
Modern Medical and Surgical Management Options
Once a severe structural blockage or megacolon is diagnosed, treatment must be carefully tailored based on the stability of the individual and the underlying root cause.
Phase 1: Conservative and Medical Decompression
For individuals who do not show immediate signs of structural damage or systemic infection, the initial goal is to safely empty and decompress the overextended bowel.
-
Clinical Enemas and Lavages: Specialized, large-volume solutions are administered in a controlled medical setting to gradually soften and flush out the dense material.
-
Manual Disimpaction: Performed under appropriate sedation or anesthesia when the impacted mass is located low in the pelvic cavity and cannot pass on its own.
-
Prokinetic Medications: Specific prescription therapies that target serotonin or acetylcholine receptors may be introduced to medically stimulate underlying smooth muscle activity.
Phase 2: Surgical Interventions
When the bowel wall has been permanently stretched beyond recovery, or if a nerve deficit is confirmed, surgical removal of the non-functioning tissue is often the most definitive and life-altering solution.
-
Subtotal or Total Colectomy: The surgeon removes the severely dilated, non-functioning sections of the large bowel. The remaining healthy segment of the small intestine is then safely reconnected to the lower tract, allowing for a return to near-normal digestive function.
-
The Pull-Through Procedure: Specifically utilized for adult Hirschsprung’s cases. The surgeon resects the narrow, nerve-deficient segment and pulls the healthy, nerve-rich upper bowel down to connect directly to the anus.
-
Temporary or Permanent Diversion: In acute emergencies where the tissue is unstable, a temporary diversion (such as an ileostomy) may be created to allow the body to heal before final reconnection takes place.
Essential Long-Term Strategies for Maintaining Optimal Digestion
For the general population looking to optimize their daily digestive health and minimize the long-term risk of developing severe, chronic retention, incorporating structural lifestyle habits is incredibly beneficial.
Structural Hydration
The large bowel acts as the body’s primary water regulator. If you do not drink adequate fluids, your body will continuously strip moisture from your stool, making it incredibly dense and difficult to pass. Aim for consistent water intake throughout the day rather than drinking large amounts all at once.
Balancing Dietary Fiber Intakes
Fiber acts as a natural bulking agent that stimulates peristalsis. However, a common mistake is drastically increasing fiber intake without adding enough water, which can inadvertently worsen a slow-moving impaction. Focus on a mindful balance of both soluble fiber (oats, avocados) and insoluble fiber (whole grains, vegetables).
Honorable Mention: Physical Activity
The physical movement of the body directly influences the movement of the gut. Regular physical activity—such as daily walking, swimming, or core-strengthening movements—mechanically stimulates the natural contractions of the intestinal tract, preventing systemic stagnation.
Respecting the Body’s Natural Cues
Ignoring the natural urge to eliminate due to a busy schedule, social anxiety, or discomfort with public facilities is a primary behavioral catalyst for long-term retention. Consistently ignoring these signals causes the rectum to adapt to higher volumes of waste, slowly blunting the natural neurological reflexes over time.
Frequently Asked Questions Regarding Severe Colonic Stagnation
Can a regular period of retention transform into a megacolon?
A brief, occasional bout of slow digestion due to travel, dietary changes, or stress will not cause a megacolon. A megacolon requires months to years of continuous, severe, unresolved retention accompanied by an underlying functional or neuromuscular vulnerability.
Is an extended abdomen always a sign of a structural blockage?
No. Abdominal expansion can be caused by regular gas buildup, fluid accumulation, food intolerances, or weak abdominal muscles. However, if the distension is accompanied by a prolonged lack of elimination, severe pain, or vomiting, it requires prompt professional evaluation.
Can the bowel return to its original shape after severe expansion?
In mild to moderate cases of functional impaction, once the blockage is safely cleared and regular habits are maintained, the smooth muscle can gradually regain some of its original tone and shape. However, in long-standing, severe megacolon presentations, the structural stretching is often permanent, making surgical intervention necessary.